Early mobility of both adults and children in intensive care units is associated with better outcomes. Clinicians at Johns Hopkins Hospital are working to improve early mobility of PICU patients through a nurse-led program that is practical and convenient.
Read the source article for this feature from
Pediatric Critical Care Medicine.
Early mobility of both adults and children in intensive care units (ICUs) is associated with better outcomes, including reduced delirium, better physical condition, fewer ventilator days, shorter length of stay, and higher functional status at hospital discharge.
1 “We know that early mobility expedites patients’ physical and mental recovery and optimizes their outcomes outside the hospital,” said Stephanie Morgenstern, MSN, APRN, ACCNS-P, CCRN, a pediatric clinical nurse specialist at Johns Hopkins Hospital in Baltimore, Maryland, USA, which is why early mobilization is a key recommendation for adults and children as part of SCCM’s ICU Liberation Bundle (A-F).
2
The ICU Liberation Bundle comprises six elements, one of which is early mobility and exercise. A 2022 survey of pediatric ICUs (PICUs) found that adherence with the early mobility element was lowest of all the six elements. Only 26% of PICUs had a guideline, protocol, or policy for early mobility.
3
“Historically, healthcare professionals have felt that keeping children immobile is the safest thing to do to prevent dislodgement of indwelling medical equipment,” explained Jessica M. LaRosa, MD, a pediatric critical care specialist at Johns Hopkins Hospital and assistant professor of anesthesiology and critical care medicine at Johns Hopkins University School of Medicine. “So it’s a big cultural shift to ask nurses to mobilize children who have a lot of small lines and tubes in them and to do so safely. A great body of literature has been dedicated to proving that it’s safe, but that body of evidence hasn’t actually translated to care at the bedside.”
The Findings
Recognizing that nurses lead 65% of mobility activities for critically ill children,
4 Dr. LaRosa and Ms. Morgenstern are leading a team at Johns Hopkins Hospital working to improve early mobility of PICU patients through a nurse-led program that is practical and convenient. Their findings were published in the January 2026 issue of
Pediatric Critical Care Medicine (PCCM).
4
In 2014, a Johns Hopkins team led by Sapna R. Kudchadkar, MD, PhD, FCCM, developed and implemented PICU Up!, the first multifaceted multiprofessional early mobility program for critically ill children.5 Dr. Kudchadkar is a leader in ICU liberation, director of the International PICU Up! Collaborative, and an author on the current
PCCM article.
4
During Dr. LaRosa’s fellowship research, she learned that one of the barriers to PICU Up! implementation was nurses’ concerns about safety. Nurses said they felt unprepared to safely move PICU children to a chair or have them walk around. Simulation appeared to be a solution. “It seemed to me like a logical transition that if you’re concerned about mobilizing a patient with a lot of lines and tubes, practicing on a mannequin felt like a safe way to do it,” Dr. LaRosa said.
In 2022, the Johns Hopkins PICU Up! team developed a simulation-based curriculum to enhance the program’s sustainability. In 2024, the team developed an in situ simulation to continue to improve implementation and sustainability.
One of the challenges of the simulation-based curriculum was that nurses had to be away from the PICU for a four-hour training period at the simulation center. While pre- and post-evaluations of the training showed it improved nurses’ knowledge, skills, and comfort level, Dr. LaRosa wanted to ensure the program would be used once the nurses returned to the PICU.
“I’m happy that the nurses feel better doing it, but what I really care about is that they actually
are doing it, and we recognized that it was probably not that feasible to have every single nurse come to a simulation center for four hours to learn this,” said Dr. LaRosa, director of the John Hopkins PICU Up! program. Therefore, the PICU Up! team decided to take the simulation directly to the nurses, showing them how to move a critically ill toddler from the bed to a pediatric mobility chair. It takes the trainer about 15 minutes to set up the simulation in an empty PICU room.
Collaborating with charge nurses to arrange unit coverage helped encourage participation. In addition, Ms. Morgenstern played a vital recruitment role as a PICU nurse who helped create and champion the simulation. “In an ICU, stepping away for even 15 minutes can sometimes feel overwhelming,” Ms. Morgenstern said. “So getting cultural support for something like that was important. I was able to tell them that it’s possible, the simulation is only 15 minutes, and we’ll get you back to the bedside as fast as we can.”
The unit has 100 pediatric critical care registered nurses, who were recruited in person and by email. Each participant received a $15 gift card. The simulation session took about 10 minutes, followed by a 5-minute debrief and a 5-minute educational presentation in which Dr. LaRosa reinforced key concepts.
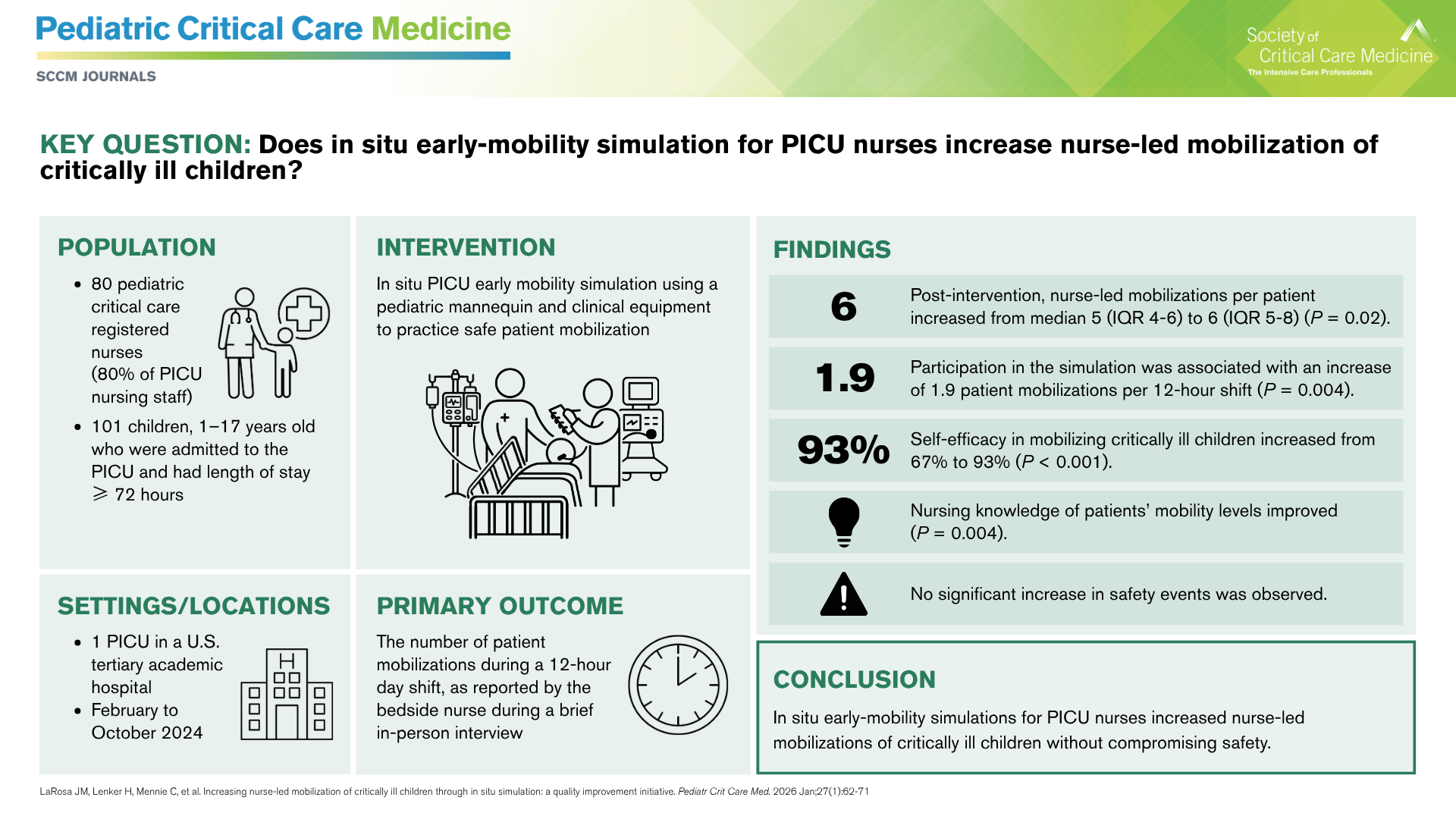
The primary outcome was nurse-reported number of mobilizations per patient in a 12-hour shift. This was collected through a 3- to 5-minute in-person interview with the patient’s nurse. Only day shifts were captured because a core focus of the PICU Up! program is sleep hygiene.
4
Of the 100 critical care nurses, 80 participated in the program from February to October 2024. Before the in situ simulation, 67% of nurses rated their self-efficacy in mobilizing a critically ill child as fairly confident or very confident. After participating in the simulation, that percentage increased to 93%.
Since the study was completed, Johns Hopkins PICU nurses have mobilized critically ill children nearly two additional times per 12-hour shift without an increase in safety events.
What’s Next
While the findings are promising, there is little research on the appropriate dose and duration of early mobility for critically ill children. Therefore, the clinical impact of two more nurse-led mobilizations per patient in a 12-hour shift is difficult to quantify.
4 One of the challenges of PICU Up! training is sustainability. A nursing shortage and high nurse turnover in the United States will require the need for simulations to be performed more frequently. “The reality of nursing turnover means that this kind of saturation of exposure is going to dwindle as people leave,” Ms. Morgenstern said.
Dr. LaRosa led all of the in situ simulations, even coming in during her off-hours to train night-shift PICU nurses. “Being able to build a program that doesn’t rely on a single person who comes in 100 times themselves is going to be important,” Ms. Morgenstern said. “I think it’s possible, but it just needs to look different for sustainability.”
The team continues to address these challenges. The PICU Up! four-hour training session is held each quarter for all onboarding nurses. The training was recently moved from the simulation center to a PICU room. The team is also developing a simulation curriculum on PICU core concepts in which nurses will lead the monthly in situ PICU Up! simulation.
In addition, a multiprofessional team now performs rounds weekly, aiming to identify barriers to implementing the ICU Liberation Bundle for high-risk children and creating a plan to address those barriers. Dr. LaRosa is applying for grants to expand the in situ simulation to other hospitals across the United States. The original PICU Up! program has been implemented directly at more than 25 U.S. children’s hospitals and adapted for more than 200 hospitals globally.
5