Communication breakdowns during patient handoffs from intensive care units (ICUs) to wards can harm patients. A recently developed low-barrier intervention, the ICU-PAUSE tool, improved these handoffs and was easily adaptable to local institutions, potentially leading to better patient care.
Read the source article for this feature from Critical Care Explorations.
Communication breakdowns during patient handoffs from intensive care units (ICUs) to wards can harm patients. A recently developed low-barrier intervention, the ICU-PAUSE tool, improved these handoffs and was easily adaptable to local institutions, potentially leading to better patient care.
Systems have been developed to improve handoffs between day shifts and night shifts within the wards, but there has been less focus on handoffs from the ICU to the wards. “The ICU-to-ward transition is one that, more recently, with our research and others, is being recognized as a high-risk time, a time that’s vulnerable for patients to have any type of medical error but particularly a diagnostic error,” said Lekshmi Santhosh, MD, MAEd, associate professor in the Division of Pulmonary and Critical Care Medicine at the University of California in San Francisco, California, USA.
The risk of errors may increase for a variety of reasons, she said, including abrupt reduction in monitoring, transition to a new team of clinicians, and diagnostic uncertainty. There are three primary categories of errors: not transmitting important information, transmitting wrong information, and not communicating when responsibility for the patient’s care will transition, according to Patrick G. Lyons, MD, assistant professor of medicine in the Division of Pulmonary, Allergy, and Critical Care Medicine at Oregon Health and Science University School of Medicine in Portland, Oregon, USA.
Handoff timing varies significantly by ICU and by hospital, Dr. Lyons said. ICUs differ widely in structure, staffing, workflows, and electronic health records (EHRs). “At some hospitals, when a patient physically leaves the ICU, that’s when the baton gets passed,” he said. “But at other hospitals, as soon as the patient’s level of care is downgraded from critically ill to ward status, the ward team takes over. Because of this heterogeneity, it’s not easy to say there’s a one-size-fits-all approach that can make that baton pass straightforward.”
Drs. Santhosh and Lyons are critical care specialists and longtime collaborators on a project to improve the ICU-to-ward handoff. They met more than 10 years ago as fellows at different institutions based on their shared passion for researching and improving handoffs. A third longtime collaborator is Juan Carlos Rojas, MD, assistant professor in pulmonary and critical care medicine at Rush University in Chicago, Illinois, USA.
The three partners developed ICU-PAUSE, an ICU-to-ward handoff tool designed to structure handoff communication. The tool is a standardized transfer note template for the EHR.
1 ICU-PAUSE, which comes with educational and implementation materials, is now being used in more than 37 hospitals across the United States and in at least one site outside the United States, according to Dr. Santhosh.
The tool is a structured rubric that leads clinicians through the information to collect, organize, and convey to the ward team. It was built with adaptability in mind and includes a dot phrase, which is a customizable shortcut for EHRs. Also included are wild card spaces that prompt clinicians to fill in more details.
The Findings
For their latest research project, the ICU-PAUSE developers tested the real-world application of the tool in diverse hospital settings.
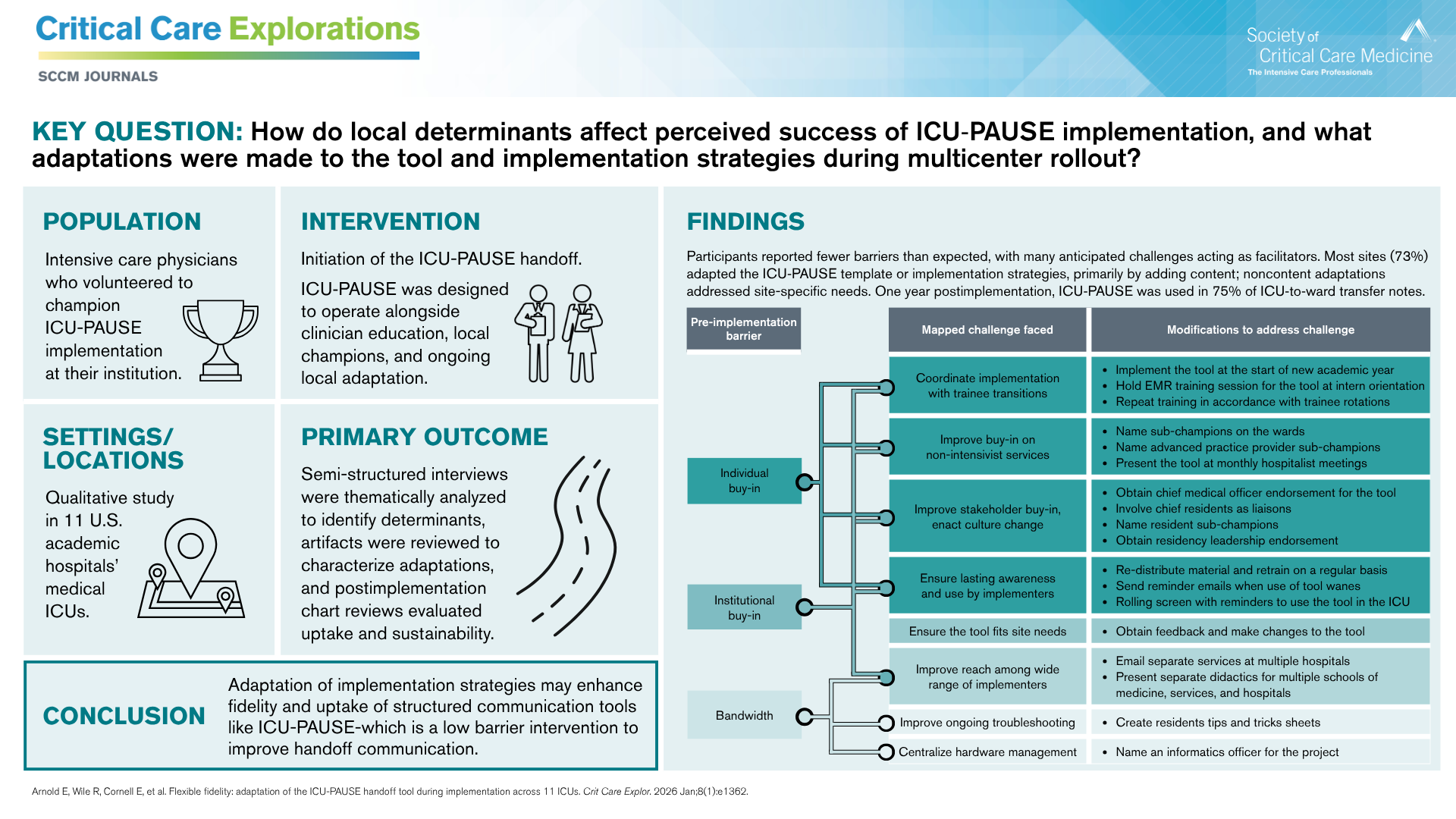
2 They conducted a multicenter qualitative study to evaluate how ICU-PAUSE was adapted during implementation at 11 U.S. hospitals in 2022. Their findings were published in the January 2026 issue of Critical Care Explorations.
2
After implementation, the investigators analyzed three areas: perceptions of the tool based on interviews with intensivist physician site champions; content, structural, and functional adaptations to the tool; and adherence to and completeness of the ICU-PAUSE template in ICU-to-ward transfer notes across sites.
Dr. Lyons noted that in many cases, what they anticipated as barriers actually turned out to be benefits. The team had hypothesized that individual and institutional buy-in, time, and technology might be key barriers. But participants appreciated the tool’s ease of implementation, use, and adaptability within their institution's EHR.
The anticipated barriers “turned out to be things we leaned on to make uptake go even better,” Dr. Lyons said. “We were concerned about IT support, but when we made the straightforward dot phrase, it turned out that’s really easy for everybody to absorb. So they didn’t need a huge rebuild of some facet of the EHR to support this project. It was something that could be done at essentially no cost.”
The tool “was easily implemented and scaled up at a diverse set of institutions across the country with high fidelity and local adaptations that helped people use it within their own local context to help them better care for the patients where they are,” Dr. Santhosh said. “The beauty of this tool is that it improves communication, it improves team collaboration, and it improves patient care by creating this shared mental model that allows the ICU team and the ward team to be on the same page cognitively.”
The investigators encourage ICU-PAUSE users to consider it a living document that they fill out in the EHR throughout a patient’s stay rather than waiting until handoff. For example, a resident who cares for a critically ill patient on day zero could describe what the initial 24 hours look like. This provides information to the next clinician, who could continue to update the rubric. Continual updating would facilitate summarization when it is time to transfer the patient to the ward.
One aspect of the tool that could be used more effectively is the to-do list section, Dr. Lyons said. Clinicians did not always use it, and even when they did, it was not used to its full potential. “We think this is the element that is the most forward-thinking.”
The to-do section takes more thinking, planning, and time for a clinician to develop an illness script, the patient’s expected course, and goals and benchmarks for continued improvement, he said. “As learners are developing those heuristics, it’s harder for them sometimes to fill this out. I think that’s especially true if there still is diagnostic uncertainty, where you may not be sure what the next set of benchmarks ought to be.” However, he said, “anything we can do to help focus the next diagnostic and therapeutic steps would give the team some guideposts along the way when the patient is transferred, and that would be ideal.”
What’s Next
ICU-PAUSE use continues to grow, including in hospitals outside the United States. In the future, the team would also like to survey frontline clinicians about their experience with the tool; the most recent interviews were with tool champions, who talked about implementation. “We don’t really know all the details of how implementation impacted day-to-day care because what we’ve heard has trickled up and been filtered through the champions. Hitting the bedside and hearing input is going to be really important,” Dr. Lyons said.
The team also wants to discover whether the tool has improved patient care and outcomes, which is ultimately the main goal. To measure this, the researchers are now evaluating a large data set from hospitals that use the tool to determine how ICU-PAUSE may have affected areas such as ICU readmissions, complications, hospital duration of stay, intermediate-term outcomes, mortality, and costs of care.
The ICU-PAUSE tool, toolkit, and resources can be accessed at no cost here.