A Society of Critical Care Medicine task force developed a core set of essential 541 skills needed to be an adult critical care specialist.
Read the source article for this feature from Critical Care Medicine
.
A Society of Critical Care Medicine (SCCM) task force has delineated the common core knowledge and skills required of all intensivists, no matter which specialty led them to critical care medicine.
In non-U.S. countries, critical care medicine is considered to be a single subspecialty. Future critical care medicine physicians complete a critical care residency after medical school or a critical care fellowship after a primary specialty residency. But in the United States, critical care medicine developed along specialty lines, which led to physicians of different specialties (e.g., anesthesiology critical care medicine, surgical critical care medicine, pulmonary critical care medicine, neurocritical care) completing a critical care fellowship in that specialty.
1
“It’s this fragmented, siloed system that was never really planned that way. In some places a surgical critical care fellow may not be able to even do an elective rotation in the medical ICU because people have siloed themselves off,” said Samuel A. Tisherman, MD, FACS, FCCM, professor of surgery, director of the Center for Critical Care and Trauma Education, and director of the surgical ICU at the University of Maryland Medical Center. However, there is significant commonality of knowledge and skills regardless of an intensivist’s primary specialty, Dr. Tisherman said.
In 2015, SCCM established the multidisciplinary Critical Care as a Specialty Task Force to review the different critical care training pathways in the United States and consider alternatives. The task force recommended that credentialing boards consider creating a common certifying examination.
1
In 2025, a different SCCM task force, the Defining Intensivist Task Force, developed the following definition of an intensivist: “a physician who has successfully completed an accredited program or equivalent critical care/intensive care medicine training and maintains advanced certification (if available); and shows dedication to the area of critical/intensive care medicine in the way of professional work.”
2
Next, SCCM created the Adult Critical Care Physician Core Knowledge and Skills Task Force, with representatives from stakeholder organizations including medical societies, member boards of the American Board of Medical Specialties (ABMS), and review committees of the Accreditation Council for Graduate Medical Education (ACGME). This task force has delineated 541 skills essential to being an adult critical care specialist. The process and list of skills were published online in
Critical Care Medicine in December 2025.
3
“What we were trying to establish was that no matter what your primary specialty, there’s this core you should have,” said Dr. Tisherman, who cochaired the task force with Antoinette “Toni” Spevetz, MD, FACP, FCCM, and J. Christopher Farmer, MD, MCCM. “Eighty to 90% of what you learn in a fellowship program is the same kind of core set. So much of what we do is the same.”
The Findings
At its first meeting, the task force agreed that the goal should be to define what every intensivist should know. “That seemed like something nobody could really argue with,” Dr. Tisherman said. “This was important for training. But there’s also a public trust side too. No matter what the training was of the person caring for you in the ICU, you should have trust that they have this core set of knowledge.”
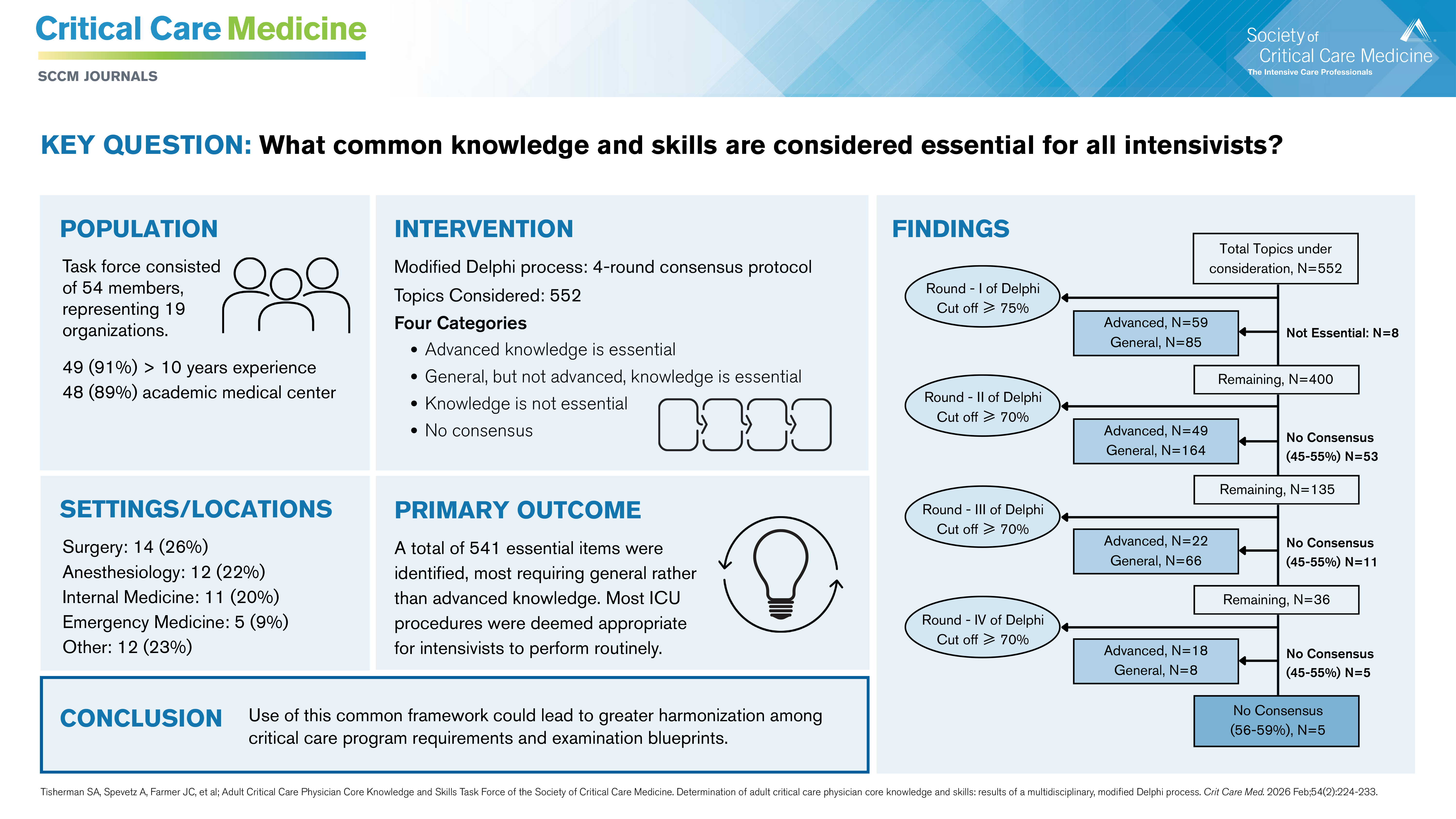
The task force developed a list of topics by reviewing the various board examination outlines and fellowship program requirements. They then used a modified Delphi method to categorize skills as advanced, general (in which the intensivist may need help from a specialist), or not essential. The participants continued through multiple Delphi rounds of voting to determine the final list. The last two rounds were discussed over video chat, with a facilitator and anonymous online voting.
Of the 541 skills, 145 were deemed to require advanced knowledge and 323 to require general knowledge. For 73 items, consensus of “advanced” versus “general” could not be achieved, but the task force still called them essential skills. Only eight items were determined to be nonessential.
“We recognize that it’s a long list, but that fits in with the notion that there is a lot required—no matter whether you’re going through surgery or medicine or anesthesia or neurology—and a lot of this is common among the specialties,” Dr. Tisherman said. “One of the basic principles of critical care as a specialty is that we are looking at the whole patient,” he added. “Yes, we may need specialists for specific things, but it’s way better to have one team, led by an intensivist, that is managing the whole patient, rather than care by committee.”
The task force also included 16 procedures in the skill set. Procedures did not fit into the advanced/general knowledge paradigm. Instead, they were categorized as “intensivist performs routinely,” “intensivist performs only in an emergency,” or “intensivist knows” about the procedure. Most of the 16 procedures were categorized as “intensivist performs routinely.”
What’s Next
Dr. Tisherman said that task force participants hope their work will spur organizations such as the ACGME and ABMS to evaluate the core skill set, with the goal of developing more homogeneity across the specialties.
“Whether this leads to more direct communication among the boards or consideration of a shared examination, I don’t know,” he said. “One of the important things is that we were able to bring together representation from not just the boards, but the ACGME and other organizations involved in critical care medicine training and critical care delivery, to talk about this. That is an accomplishment we’re proud of and hopefully one that will lead to continuing conversations.”