


New from Critical Care Medicine, Clinicians Corner explores a patient case that has sparked debate. Review the case details, vote on how you would treat the patient, and after you submit, see how current poll results are trending. Then watch for an email with access to the Critical Care Medicine article featuring authors’ in-depth perspectives on the case.
Look for the next poll in June!
A 52-year-old woman presents to the emergency department with a 1- to 2-day history of fever, right flank pain, and nausea. Vital signs are: temperature 39.1 °C (102.4 °F), heart rate 130 beats/min, respiratory rate 22 breaths/min, and blood pressure 70/40 mm Hg. She has right costovertebral angle tenderness. Laboratory findings are: WBCs 15 × 103/μL, creatinine 1.9 mg/dL, and lactate 3.5 mmol/L. Urinalysis reveals many WBCs and few RBCs. CT reveals right hydronephrosis with an obstructing ureteral stone. She receives 2 L lactated Ringer solution and is started on norepinephrine and broad-spectrum antibiotics. Blood and urine cultures are pending. Urology plans intervention once the patient is stabilized. Despite increasing norepinephrine to 0.25 µg/kg/min, blood pressure remains low at 80/50 mm Hg.
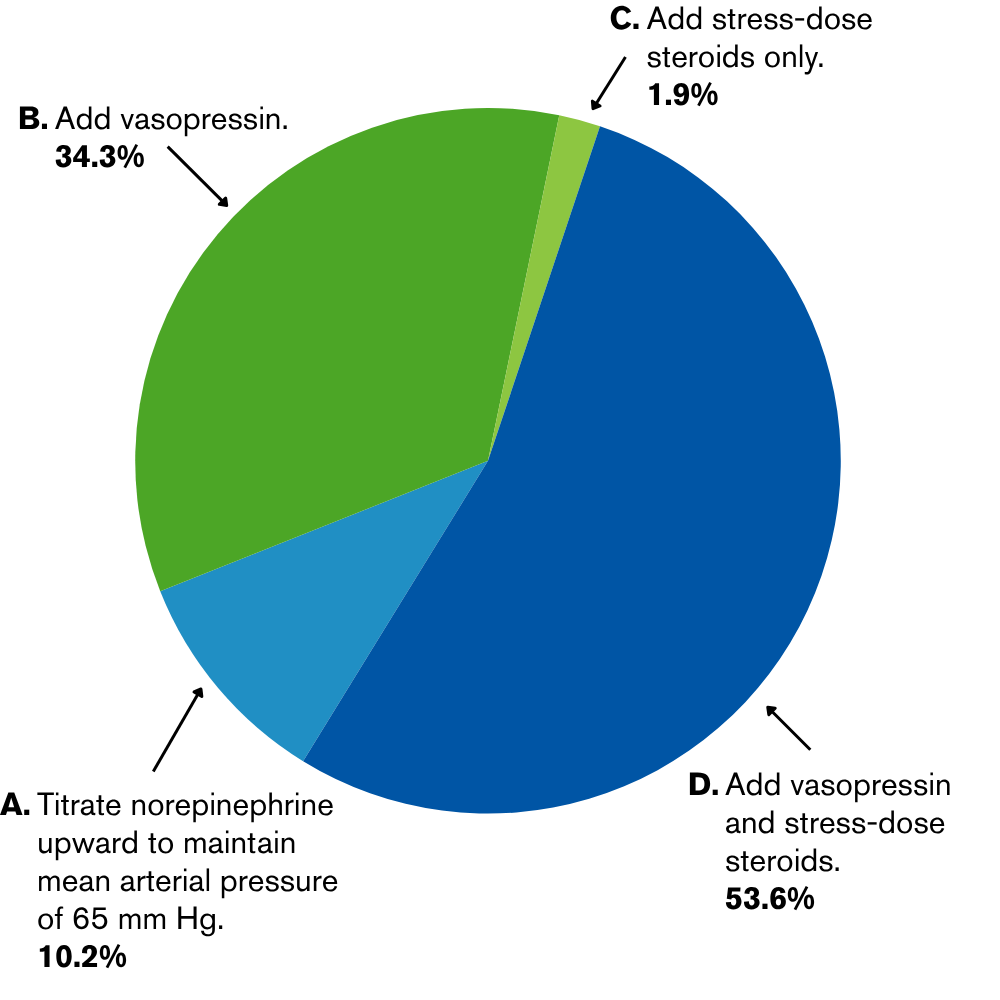
Which of the following is the most appropriate next step?
Here’s how your peers responded:
Read the research: Clinicians Corner: Practical Tips for Clinical Stabilization in Septic Shock


